Clinical Photos & Pearls
With today’s advanced technology and surgical techniques, the following mild complications after Lasik are far less common than they used to be but still occur and need to be properly managed.
Here are some images as well as the proper protocols for review.

Epithelial Ingrowth
This rarely occurs post initial flap creation.
Every ingrowth case I’ve managed was after a lift for a LASIK enhancement and the vast majority of those cases were after a lift of a microkeratome created flap. Very few were after a lift on an Intralase case but still occur and may need to be managed. Below are some images of ingrowth. The protocol would depend on the size and location of the ingrowth nest. Although not an urgent issue, if any ingrowth is noted centrally (fig A), within the line of sight, a referral back to the center is advised as it will most likely need to be surgically removed via a flap lift and rinse. If the ingrowth is located near the edge of the flap (fig B), the size of the nest is small with defined margins, and there are no visual symptoms or discomfort, you can simply monitor Q 2-4 weeks looking for progression or signs of flap melt. If progression is noted, unexplained residual cylinder seen or BVA is reduced then even peripheral ingrowth should be referred back for an eval. As always, don’t hesitate to refer back to our center if unsure of anything.
Fig A
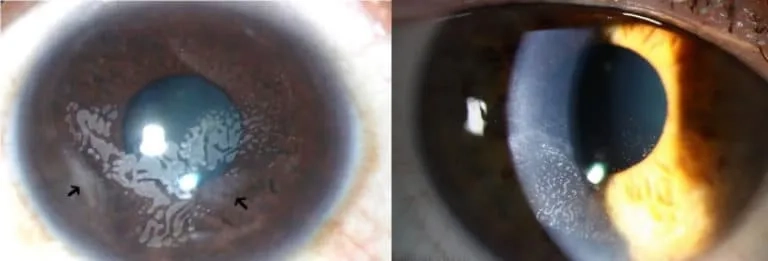
Fig B
Diffuse Lamellar Keratitis
Diffuse Lamellar Keratitis is a sterile inflammatory reaction to exotoxins after a flap is created during LASIK.
Onset is generally within 48 hrs to 1 week after the procedure but rarely can occur a few weeks later. Clinical presentation is usually a diffuse or multifocal accumulation of neutrophils often called “Sands of the Sahara” due to its desert like appearance.
There are 4 stages of severity listed below:
- Stage 1: Cells infiltrate the periphery of the flap, without involving central cornea.
- Stage 2: Peripheral cells migrate to the center of the cornea, and impair vision; presentation is usually 2 to 3 days after surgery.
- Stage 3: Cells at the central cornea form clumps of dense cell aggregates.
- Stage 4: Otherwise known as central toxic keratopathy, stage 4 characteristically has no inflammatory cells at the anterior chamber or cornea, but there is a central stromal necrosis, and the cornea becomes opacified; onset is usually 3 to 9 days after refractive surgery.
The vast majority of DLK cases encountered are Stages 1 and 2 (fig C). Typically, the best way to treat this complication is aggressive use of Pred Forte Q1-2hrs while awake until improvement is noted, followed by a slow taper over the next month until full resolution is seen. This is to avoid a rebound reaction and most cases of DLK resolve within 2 -4 weeks of diagnosis. The sooner the treatment is started, the better the prognosis and the quicker the resolution. If the appearance looks far denser or opacified (fig D), this should be referred back to our office for evaluation as stage 3-4 could lead to Central Toxic Keratopathy which is much more difficult to treat.
Fig C
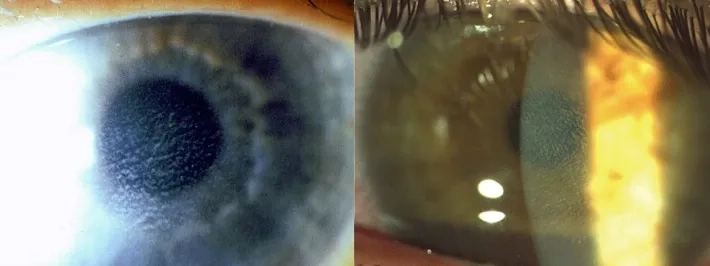
Fig D

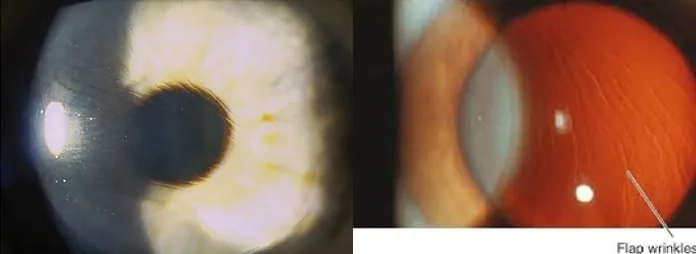
Striae
These are full flap thickness wrinkles caused by rubbing the eyes.
These are usually seen within the first few days of surgery and generally present with positive visual symptoms like blur, glare and/or decreased BVA but without discomfort. Occasionally you will see what looks like tiny striae but present without any visual symptoms at all. These are microstriae and typically seen after Lasik on high myopic patients (fig E). These are usually benign and rarely need surgical intervention. Macro or full striae require surgical intervention to lift and smooth out the striae (fig F). The prognosis for recovery is very good, especially if treated within the first 2 weeks of surgery. Delay in lifting can result in permanent problems so timely referral is important.
Fig E
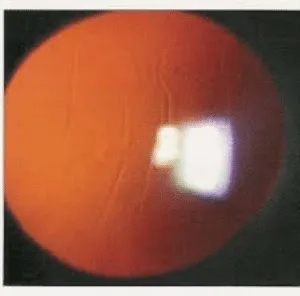
Fig F
Displaced Flap
If the flap is dislodged in any way, pain, decreased vision and tearing are the hallmark signs and this always requires surgical intervention to fix.
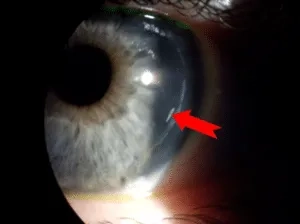
Upon looking at the edge you will notice a gap between the flap and edge and usually also see overlap on the opposite side (fig G). Typically, the visual recovery will be slower in that eye and will need to stay on the same drop regimen that was instilled during the original treatment. Prognosis is usually very good for complete recovery. I have also posted an image of an abrasion so you will be able to differentiate between a true full flap dislodgment vs an epithelial abrasion. The best way to tell the difference is to view the surface in the area of the abraded/dislodged flap. A flap dislodgement will appear pitted or like an orange peel (fig G); whereas, an abrasion will appear as a smooth/clear surface (fig H).
Fig G
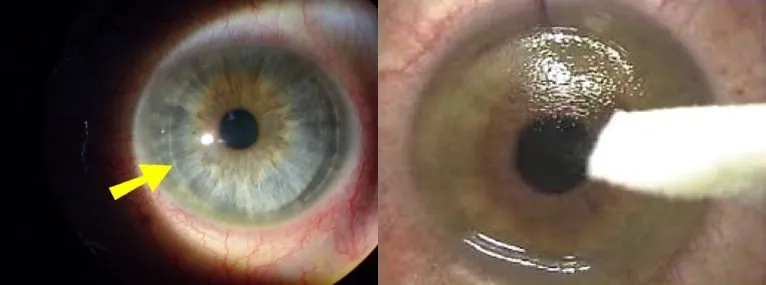
Fig H
